MNCM’s President & CEO Liz Cinqueonce Joins Great Lakes Executive Leadership Council Advances Regional Collaboration and Quality Improvement

MN Community Measurement Recognizes Innovation and Collaboration in Clinical Quality Measurement
MN Community Measurement (MNCM) has released two new reports highlighting the state’s health care performance: Health Care in Minnesota: Summary Report on Quality, Disparities, and Cost and Health Care in Minnesota: Health Care Quality Leaders . Together, these reports provide a comprehensive analysis of 2024 data, examining trends in health care quality, disparities, and costs, while also recognizing medical group quality leaders and those demonstrating meaningful improvement. These reports, based on data submitted to MNCM in 2025 and reflecting care delivered in 2024, work in tandem with MNCM’s Performance Hub —an interactive platform providing statewide analyses of health care quality and cost measures. Collectively, these tools equip community partners, including medical groups, payers, policymakers, public health agencies, researchers, and community-based organizations, with actionable insights to drive improvements in care and advance health equity across Minnesota. Report highlights include: Health Care Quality Significant gaps remain in asthma control, with thousands of patients needing improved care to meet statewide benchmarks. Colorectal cancer screening rates for the newly eligible 45-49 age group continues to improve. While the 2024 rate for all age groups has significantly increased compared to 2023, it remains significantly lower than 2021. Childhood immunization continues to show a decrease in statewide rate from year to year. This measure has not shown improvement in rates following the COVID-19 pandemic. There were modest improvements in breast cancer screening, cervical cancer screening, controlling high blood pressure, diabetes eye exams, and immunizations for adolescents. Health Care Disparities Black, Indigenous, Multi-Race, and Hispanic/Latinx patients experienced the most disparities across multiple measures, particularly in Colorectal Cancer Screening. Patients speaking Somali and Spanish, as well as those from Laos, Mexico, and Somalia, had lower rates of preventive care and chronic disease management compared to statewide averages. Cost and Utilization The total cost of care increased by 7.3% in 2024, primarily driven by an 8.9% rise in pharmacy costs and an 8.3% rise in professional fees. All categories of medical services saw increased use, except for inpatient admissions. Women aged 36-64 had the highest number of claims, while men aged 18-35 had the lowest number of claims. Quality Leaders In 2024, 31 medical groups were recognized as quality leaders across the measures reported by medical groups. In 2024, 58 medical groups were recognized as quality leaders across the measures reported by payers.
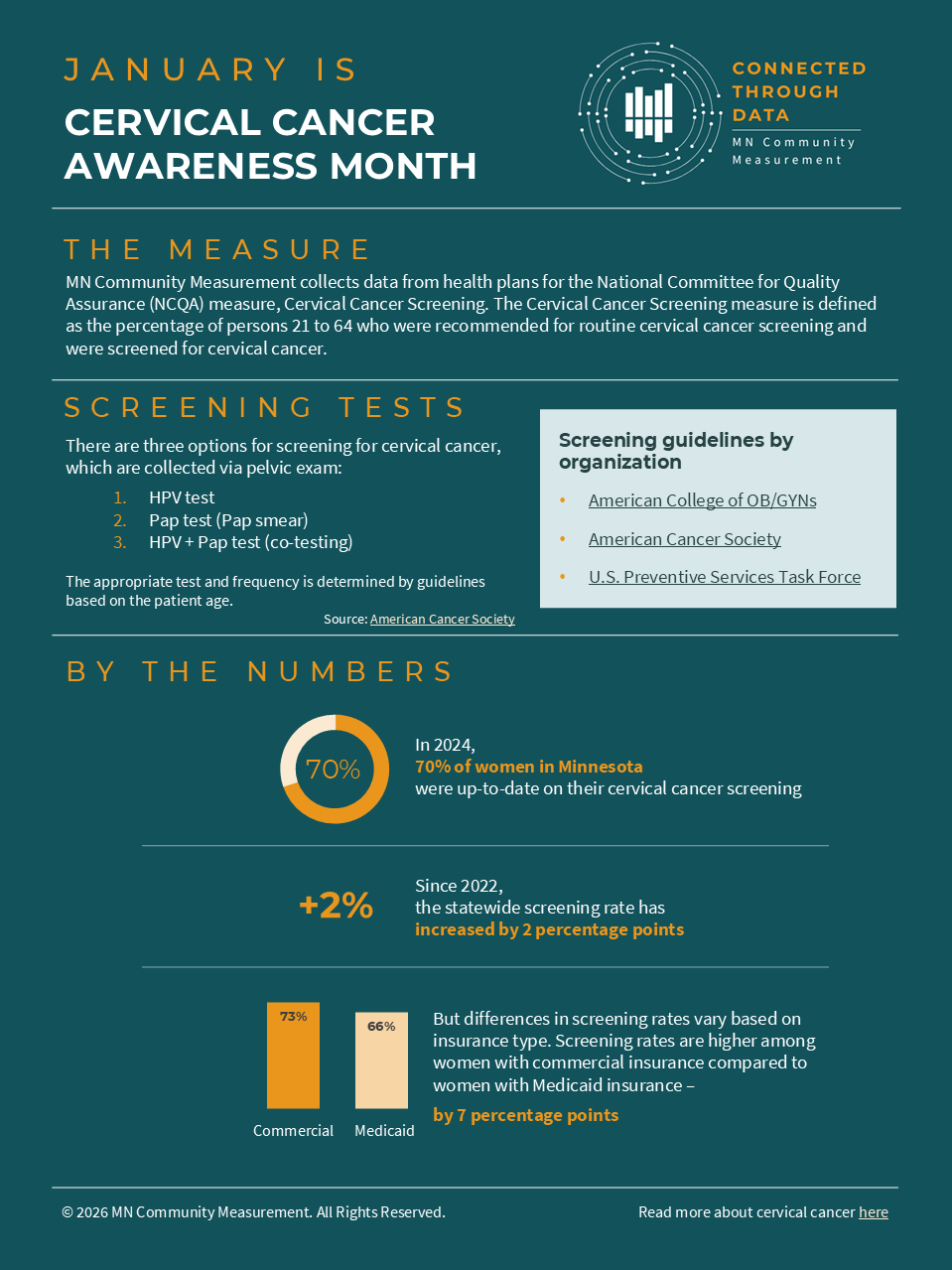
CONNECTED THROUGH DATA: Uncovering Disparities in Cervical Cancer

This October marks the 40th anniversary of Breast Cancer Awareness Month. According to the American Cancer Society, about 1 in 8 women will be diagnosed with invasive breast cancer in their lifetime. Fortunately, however, early detection through screening and advances in treatment have decreased mortality by 44% since 1989. Screening can catch cancer early, when it is…
The post Empowered by Data: Uncovering Screening Disparities and Reducing Breast Cancer Risk appeared first on MN Community Measurement.